






 - Government of India")
 - Government of India")

")


")



Urban Malaria Scheme(UMS)
BackINTRODUCTION
CONTROL OF MALARIA IN URBAN SITUATION
 Malaria in urban areas was considered to be a marginal problem restricted to mega towns only and was considered that local bodies are capable of handling it. Therefore while launching the National Malaria Eradication Programme in 1958, Urban Malaria was not included. By 1970s, incidence of rural malaria came down drastically i.e. 0.1 to 0.15 million cases per year but the urban town reported rising trend. Madhok Committee in 1970, investigated the problem and assessed that 10 to 12% of total cases were contributed by urban areas. The committee recommended anti larval measures for containment of urban malaria, because it was feared that proliferation from urban to rural may spread and nullify the gains already made.
Malaria in urban areas was considered to be a marginal problem restricted to mega towns only and was considered that local bodies are capable of handling it. Therefore while launching the National Malaria Eradication Programme in 1958, Urban Malaria was not included. By 1970s, incidence of rural malaria came down drastically i.e. 0.1 to 0.15 million cases per year but the urban town reported rising trend. Madhok Committee in 1970, investigated the problem and assessed that 10 to 12% of total cases were contributed by urban areas. The committee recommended anti larval measures for containment of urban malaria, because it was feared that proliferation from urban to rural may spread and nullify the gains already made.
HISTORICAL BACKGROUND
The control of malaria in the urban areas was thought of an important strategy as a programme complimentary to the NVBDCP for rural areas. Modified Plan of Operation (MPO) was designed and submitted to the Cabinet to tackle the malaria situation in both urban and rural areas in the country simultaneously. Under MPO, it was decided to initiate anti-larval and anti-parasitic measures to abate the malaria transmission in urban areas. The proposal to control malaria in towns named as Urban Malaria Scheme was approved during 1971 and it was envisaged that 131 towns would be covered under the scheme in a phased manner. This scheme was sanctioned during November, 1971 and the expenditure on this scheme is treated as plan expenditure in centrally sponsored sector. The central assistance under this scheme was treated 100 per cent grant to the State Governments in kind.
At present, Urban Malaria Scheme is protecting 142.9 million population from malaria as well as from other mosquito borne diseases in 131 towns in 19 States and Union Territory.
OBJECTIVES
The main aim is the reduction of the disease to a tolerable level in which the human population can be protected from malaria transmission with the available means.
The Urban Malaria Scheme aims at :
a) To prevent deaths due to malaria.
b) Reduction in transmission and morbidity.
NORMS
- The towns should have a minimum population of 50,000.
- The API should be 2 or above.
- The towns should promulgate and strictly implement the civic by-laws to prevent/eliminate domestic and peri-domestic breeding places
URBAN MALARIA SITUATION:
Epidemiological and disease specific background
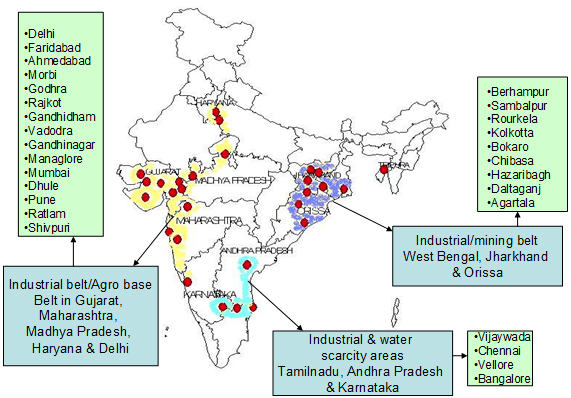
About 10% of the total cases of malaria are reported from urban areas. Maximum numbers of malaria cases are reported from Chennai, Vishakapatnam, Vadodara, Kolkata, New Mumbai, Vijayawada etc. The comparative epidemiological profile of malaria during 2005-2019 in all urban towns of the country is as follows:
| Comparative Epidemiological profile of malaria in 19 States under UMS during 2005-2021 | |||||||
| Year | Population | Total cases | P.f | P.F % | SPR | SFR | Deaths |
| 2005 | 102423064 | 135249 | 14905 | 11.02 | 2.33 | 0.26 | 96 |
| 2006 | 105782505 | 129531 | 17278 | 13.34 | 2.07 | 0.28 | 145 |
| 2007 | 112448027 | 102829 | 18038 | 16.82 | 1.92 | 0.32 | 125 |
| 2008 | 113334073 | 113810 | 18963 | 13.42 | 1.66 | 0.22 | 102 |
| 2009 | 114699850 | 166065 | 31134 | 18.75 | 2.98 | 0.56 | 213 |
| 2010 | 115159555 | 74908 | 7587 | 18.75 | 2.98 | 0.56 | 31 |
| 2011 | 130316971 | 142502 | 13910 | 9.77 | 2.07 | 0.21 | 147 |
| 2012 | 130329138 | 82554 | 8236 | 9.98 | 1.35 | 0.14 | 69 |
| 2013 | 131279000 | 65568 | 5463 | 8.33 | 1.04 | 0.09 | 26 |
| 2014 | 133857000 | 142376 | 10343 | 7.2 | 1 | 0.08 | 21 |
| 2015 | 148181952 | 28821 | 2679 | 9.29 | 0.38 | 0.035 | 17 |
| 2016 | 107953339 | 23374 | 1873 | 8.01 | 0.39 | 0.031 | 16 |
| 2017 | 117940161 | 9292 | 756 | 8.13 | 0.24 | 0.02 | 20 |
| 2018 | 116965378 | 26105 | 1721 | 6.59 | 0.68 | 0.04 | 6 |
| 2019 | 137391947 | 31735 | 1606 | 5.06 | 0.42 | 0.02 | 2 |
| 2020 | 141759779 | 17038 | 1938 | 11.37 | 0.49 | 0.06 | 1 |
| 2021 |
142595106 | 26747 | 7961 | 29.76 | 0.59 | 0.18 | 0 |
Control Strategies under Urban Malaria Scheme:
Under the scheme, Malaria Control strategy will comprise of (i) Parasite control & (ii) Vector control
- Parasite control: Treatment is done through passive agencies viz. hospitals, dispensaries both in private & public sectors and private practitioners. In mega cities malaria clinics are established by each health sector/ malaria control agencies viz. Municipal Corporations, Railways, Defence services
- Vector control comprises of the following components
- Source reduction
- Use of larvicides
- Use of larvivorous fish
- Space spray
- Minor engineering
- Legislative measure
The control of urban malaria lies primarily in the implementation of urban byelaws to prevent mosquito breeding in domestic and peri-domestic areas, or residential blocks and government/commercial buildings, construction sites. Use of larvivorous fish in the water bodies such as slow moving streams, lakes, ornamental ponds, etc. is also recommended. Larvicides are used for water bodies, which are unsuitable for use of larvivorous fish. Awareness campaigns are also undertaken by Municipal Bodies/Urban area authorities.
The control measures recommended under UMS are as below:
a. Source reduction (Guidelines for Source Reduction)

- Environmental methods of controlling mosquito breeding including source reduction minor engineering works, by filling ditches, pits, low lying areas, streamlining, canalizing, desilting, deweeding, trimming of drains, water disposal and sanitation, emptying water containers once in a week and observing weekly Dry Day etc.
b. Anti-larval methods
Chemical
- Recurrent anti-larval measures at
weekly intervals
- with approved chemical larvicides to control the vector mosquitoes are recommended. The following chemical larvicides are used in the Urban Malaria Scheme programme:
- Temephos
- Bti (WP & 12 AS)
Biological Control (Guidelines for Larvivorous fish)
In some urban areas larvivorous fish like Gambusia and Guppy are also used in certain situations where the chemical control is not feasible. Biological larvicide, Bacillus thuringiensis israelensis either wettable powder or aqueous suspension are also used for control of aquatic stages of vector mosquitoes.



Aedes larvae Anopheles larvae Culex larvae


Gambusia affinis Poecilia reticulata (GUPPY)
- Aerosol Space Spray
- Space spraying of pyrethrum extract (2%) in 50 houses in and around every malaria and dengue positive cases to kill the infective mosquitoes is recommended.
High Risk towns:
Emerging Problem of Malaria in Urban Areas
- The proportion of urban population to the total population has increased in the last few decades. This has been triggered by rural “push” (for earning livelihood and “urban pull” (for availibbng both medicare/ education opportunities) phenomenon.
- Haphazard and unplanned growth of towns has resulted in creation of “urban slum” with poor housing and sanitary conditions promoting vector mosquito breeding potential for malaria, filaria and dengue fever/ Dengue haemorrhagic fever.
- Restricted water supply has led to water storage practices in artificial containers which have generated breeding potential of An.stephensi vectors of urban malaria and Aedes aegypti, the vector of DF/DHF.
- With rapid growth of population in urban towns, existing staff strength has not corresponding strengthening and is therefore inadequate for service delivery.
- Anti-larval activities are restricted to chemical control. The focus is not on integrated source reduction measures.
- Towns not under UMS are also contributing maximum malaria cases in Mangalore.
- Due to population pressure all cities are expanding and parallel cities have come up and epidemic situations prevail. Gurgaon, Navi Mumbai, Noida.
- Old villages in expanding urban centres were kept out of overall development (sullage & sewage disposal) with unrestricted land use maintain high mosquitogenic potential.
- Development project activities without health impact assessment have resulted in malaria outbreaks in short terms and endemic malaria with foci of P.falciparum resistance strains in long term.
- Inadequate trained man-power for Control of Vector Borne Diseases.









